



















Triathlon Fueling Guidelines
Sports Dietitian Bob Seebohar was the personal sports dietitian for the 2008 U.S. Olympic Triathlon team and takes a cutting-edge approach to nutrition with his Metabolic Efficiency
Foot pain top of foot is that sharp, annoying ache that starts as a whisper after a long Sunday run and before long is loud enough to ruin a session. If it’s happening to you—especially while training for the Sydney Marathon, Gold Coast Marathon or Ironman Cairns—this practical, coach-first guide shows exactly what to test, how to treat it, and the training adjustments to stop it from coming back.
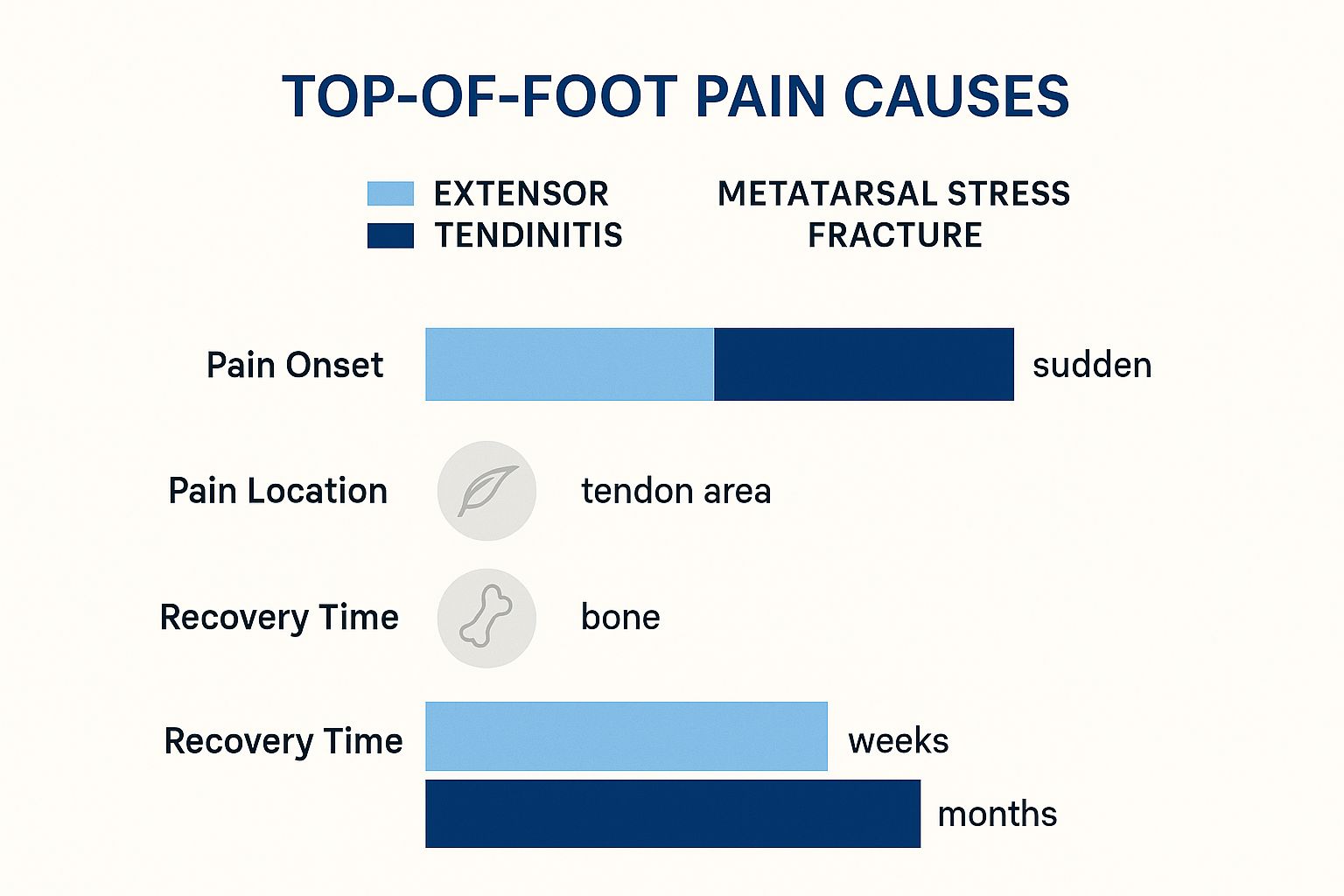
Most top-of-foot problems in runners fall into two camps: soft-tissue overload (extensor tendinitis) or bone stress (metatarsal stress fracture). Both can be painful, but they behave differently — and the management is different. Start with the simple checks below to triage the issue.
Every stride is an impact. On hot, hard Aussie roads or long coastal pavement runs, that impact adds up. Combine that with aggressive training blocks for local events (Sydney, Melbourne, Gold Coast) and narrow or worn shoes, and you have a perfect setup for overload at the top of the foot.
“Repetitive impact + direct pressure (lacing/shoe) + rapid load increases = tendon overload.” — practical checklist for making training decisions.
Play detective before panic. The aim is to determine whether you can manage this at home or whether you need imaging and a clinician.
What to do (trackside): immediately relace to create a pressure-free window over the tender area (skip those eyelets), reduce load (no hills or speed), ice 18 minutes, and swap to zero-impact cross-training (swim/cycle).
Why it works: removing pressure and reducing repetitive dorsiflexion lowers tendon friction and inflammation, while cross-training preserves aerobic fitness without impact.
How to apply (this week): replace your scheduled hill session with 40–60 minutes steady cycling at RPE 5–6 or 30–40 minutes of continuous swimming intervals (10×100m with 20–30s rest). Reassess pain after 7–10 days.
What to do: stop running immediately. See a sports clinician for assessment and imaging (X-ray or MRI). Use crutches or a controlled walking boot if recommended.
Why it works: bone healing needs unloading — continued impact risks conversion to a full fracture and months out.
How to apply: switch to pool running or an aquatic program for fitness maintenance, and plan a conservative 6–8 week non-impact block before a progressive return-to-run protocol as guided by your clinician.

| Condition | What it feels like | Common triggers (Aussie context) |
|---|---|---|
| Extensor Tendinitis | Dull, diffuse ache across top of foot; swelling; worse with running and lacing pressure. | Aggressive lacing for long runs; sudden mileage/hill spikes; narrow shoes during humid summer runs. |
| Metatarsal Stress Fracture | Sharp, localised pain; worse during/after runs; worse at rest in advanced cases. | Rapid load increase, low energy availability, worn shoes on hard surfaces. |
| Nerve Compression | Burning/tingling; sense of rubbing/pebble in shoe. | Narrow toe box shoes; swelling during long humid runs. |
When it hurts now, act smart. Below is a field-tested, step-by-step plan to reduce pain fast and keep your training productive.
If pain sits under the tongue of your shoe or under the laces, try this immediately:
What to expect: immediate reduction in localized pressure and, in many runners, a noticeable drop in pain within one run or walk.
Fixing acute pain is phase one. Phase two is building tolerance so you don’t return to the same problem when training load increases.
Every exercise below follows the UCAN 3-layer test: what to do — why it works — how to apply.

What to do: get a gait analysis at a speciality running store; test shoes with socks and orthotics you’ll use on race day.
Why it works: a shoe that matches your biomechanics reduces shear and pressure on the extensor tendons and evenly distributes load across the metatarsals.
How to apply: track shoe mileage — replace shoes at ~500–800 km depending on your weight, terrain and shoe model. If you’re switching brands or models, run a progressive 2–3 week adaptation (short runs first).
Coach’s note: dead shoes and inconsistent footwear are among the fastest routes to recurrence.
The simplest rule that works: manage weekly load increases. A pragmatic approach is a 10% weekly increase cap on running volume, but apply common sense — reduce when you add speed/hills.
Practical example: if your Base Week is 30 km, keep week-to-week increases to ~3 km (10%). If you add hill sprints or a track session, keep total km the same and replace an easy run instead of adding extra distance.
Nutrition is part of the rehab toolbox. If you’re underfuelled, tissue repair slows — tendons and bone don’t get the substrate they need.
Low energy availability impairs connective tissue repair and increases risk of stress injury. Steady energy during long sessions helps maintain form; better form = less abnormal load to the top of the foot.
There’s a point where self-management is not enough. Recognise it early and save weeks of frustration.
Podiatrist: start here if you suspect a bone issue, neuroma or need orthotics / imaging. Physiotherapist: choose this route for biomechanical chain issues (hip weakness, running form) and progressive rehab programming. Both professions often work together for a faster, safer return to running.
Short answer: no. Pain is an alarm. Running through clear signs of tendon overload or possible bone stress risks a longer layoff. Manage early and conservatively.
Depends on diagnosis. Mild extensor tendinitis: 1–3 weeks with immediate modification and rehab. More severe tendinitis: 4–6+ weeks. Metatarsal stress fracture: typically 6–8 weeks non-impact, then progressive return (clinician-guided).
No. Shoes should lock the heel and midfoot while leaving room at the front. If you feel direct pressure across the dorsum during runs, address lacing and shoe width immediately.
Yes — when the top-of-foot pain is secondary to a larger biomechanical problem (flat feet, poor arch support, abnormal load distribution). Use a podiatrist to determine if temporary orthoses or custom orthotics are appropriate.
[1] Brukner P, Khan K. Clinical Sports Medicine. 5th ed. McGraw Hill, 2017. (tendon overuse and load management principles.)
[2] Nigg BM, et al. Biomechanics and running shoes: the role of loading and cushioning in injury. Br J Sports Med. 2015.
[3] Taunton JE, et al. A retrospective case-control analysis of 2002 runners with stress fractures. Clin J Sport Med. 2002.
[4] University of Melbourne. Centre for Health, Exercise and Sports Medicine — Prevalence and impact of foot pain in the Australian population. 2019.
[5] Sports Medicine Australia. Running Injuries Fact Sheet. 2021.

 14Aug
14Aug  14Aug
14Aug  14Aug
14Aug  24Jan
24Jan  15Aug
15Aug  16Aug
16Aug
Comments are closed